Dr. Williams' Urology Resource
A Guide to Men's Health, Reproductive Medicine, and Microsurgery
Sperm Retrieval
For couples who desire a pregnancy after a vasectomy procedure, an alternative to vasectomy reversal is sperm retrieval in conjunction with In Vitro Fertilization (IVF) with Intracytoplasmic Sperm Injection (ICSI).
This is an ideal choice for couples in whom there are significant female factor infertility issues such advanced maternal age or ovavian/tubal problems.
In such cases, IVF/ICSI may be required to get pregnant, and a simpler approach than microsurigcal vasectomy reversal is to retrieve sperm from the epididymis or testis and use them for IVF/ICSI.
Sometimes a couple will request sperm retrieval to be performed with Intra-Uterine
Insemination (IUI), as this is not very invasive and appears to be the least costly
alternative for getting pregnant after a vasectomy. However, IUI can ONLY be
performed with fully mature sperm from the ejaculated semen, and the success is highly dependent on having adequate numbers of motile sperm present (>10 million).
Unfortunately, sperm retrieved from the epididymis and testicle are not mature enough or adequate in quantity to get pregnant with this form of assisted reproduction.
In fact, attempts at even performing conventional IVF with testicular or
epididymal sperm have been met with such poor success that most IVF centers today
will only perform the more sophisticated ICSI procedure in cases where epididymal or testicular sperm is present, as is always the case after a vasectomy.
Sperm Retrieval Techniques
The specific sperm retrieval technique employed depends on a number of factors including whether or not a man has obstructive azoospermia, i.e. after a vasectomy or in the setting of absent vas deferens, or non-obstructive azoospermia where there is impaired sperm production.
- Testicular Sperm Extraction (TESE)
- Testicular Sperm Aspiration (TESA)
- Percutaneous Epididymal Sperm Aspiration (PESA)
- Microscopic Epididymal Sperm Aspiration (MESA)
- Microdissection-TESE
- Vasal Sperm Aspiration
Microsurgical Epididymal Sperm Aspiration
In the setting of obstructive azoospermia (no sperm in the semen due to a blockage in the reproductive tract), sperm production is typically normal. Obstructive azoospermia can be due to ejaculatory duct obstruction, congenital bilateral absence of the vas deferens (as is seen in men with cystic fibrosis), epididymal obstruction, or most commonly vasectomy. MESA is an outpatient, same-day procedure, performed under a general anesthetic with an operating microscope through a small ~2-3cm scrotal incision. Once sperm are obtained from the epididymal fluid, they are cryopreserved (frozen) and can be used at any time in the future for IVF/ICSI.

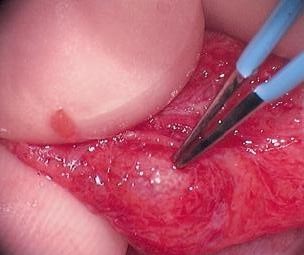
Here, the testicle (white) and obstructed epididymis (yellow) are seen.
 Next, the dilated epididymal tubules are opened with an opthalmological blade. The epididymal fluid is aspirated into a syringe using an angiocath tip. The fluid is examined for the presence of motile sperm and then sent to the andrology laboratory for cryopreservation.
Next, the dilated epididymal tubules are opened with an opthalmological blade. The epididymal fluid is aspirated into a syringe using an angiocath tip. The fluid is examined for the presence of motile sperm and then sent to the andrology laboratory for cryopreservation. Next, the area where the obliterative MESA was performed is cauterized using a needle-tipped bovie.
Next, the area where the obliterative MESA was performed is cauterized using a needle-tipped bovie.
 The 2-3cm scrotal incision is closed with absorbable sutures.
The 2-3cm scrotal incision is closed with absorbable sutures.Click here to watch Dr. Williams perform a microsurgical epididymal sperm aspiration
Microdissection Testicular Sperm Extraction
In the setting of non-obstructive azoospermia (no sperm in the semen due to low or absent sperm production), there is about a 50% chance of findings sperm by performing a microdissection testicular sperm extraction. This is a highly technical procedure and should be performed only in the hands of an experienced microsurgeon. Microdissection-TESE is an outpatient, same-day procedure, performed under a general anesthetic through a small ~2-3cm scrotal incision.

Here the testicle has been delivered into the operative field through a small incision. The testicle is the white structure at the bottom. The epididymis is the curved pink structure above the testicle. The yellow is a small amount of normal fatty tissue that protects the testicle and epididymis. When normal spermatogenesis is present, sperm exit the testicle and enter the head of the epididymis (right side of the picture). They travel through the epididymis (in this case from right to left) and then enter the vas deferens as they leave the tail of the epididymis (not shown). In this case, the testicle is small and atrophic.

The tunica albuginea is opened transversely along the equator of the testicle. Use of the operating microscope allows for excellent visualization of vital structures and lowers the risk of any damage to the testicle. Once the testicle is opened, a large surface area of tissue can then be safely inspected for areas of active spermatogenesis. The microsurgeon holds the testicle while the assistant uses irrigation (shown above) for optimal visualization.
Here, high-power optical magnification with the operating microscope allows for identification of prominent seminiferous tubules (pale yellow structures at the tip of the instrument). There is a higher chance of having active spermatogenesis in these areas. Small pieces of tissue are then handed over to the andrologist in the operating room who examines the tissue under a bench microscope. If sperm are found, they can then be used for in-vitro fertilization with intracytoplasmic sperm injection.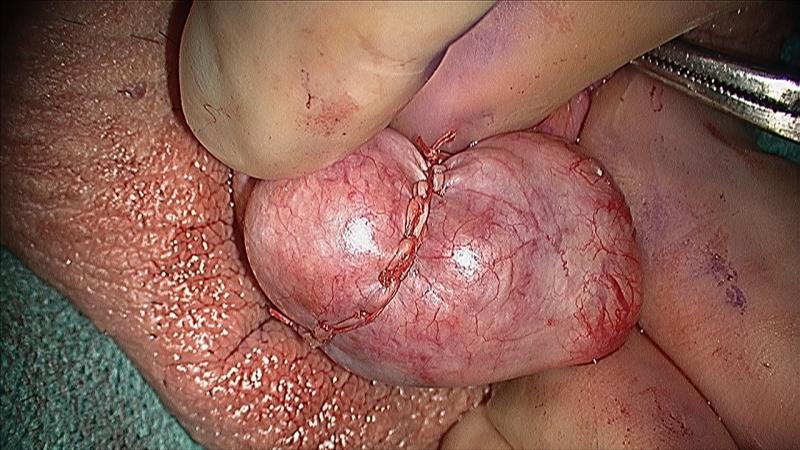
The testicle is closed with fine suture material. With this microsurgical approach, only a small amount of testicular tissue is removed, minimizing any long-term compromise to testicular function. Testosterone production by the testicles is largely unaffected by this procedure.
Dr. Williams' Article on IVF/ICSI and Male Infertility