Dr. Williams' Urology Resource
A Guide to Men's Health, Reproductive Medicine, and Microsurgery
Male Infertility
Million of couples in the U.S. are faced with infertility every year. A fraction of the women in these couples will be evaluated for infertility, and of these infertile women, only 20% of their partners will receive a medical evaluation for infertility.
Despite a male factor being present in up to 50% of infertile couples, a formal male infertility evaluation is often overlooked. There are a variety of reasons why this occurs including:
- Access to expert fertility care
- The limited number of urologists who are trained to treat male infertility
- Perception in both the public and medical communities that the problem is always due to the female partner
- The success of assisted reproductive technologies
Infertile couples are encouraged to journey through the infertility process together. In doing so, the man and the woman can gain a better understanding of the potential factors involved with both male and female infertility, and provide each other with the emotional support through these challenging and stressful periods of their lives.
Simultaneous evaluations of both the man and the woman by experts in male and female reproductive medicine can oftentimes result in more timely and cost-effective strategies that treat the infertile couple as a whole and help them accomplish their goals.
Goals of a Male Infertility Evaluation
- Identify potentially correctable conditions that if treated may allow for conception through intercourse
- Identify irreversible conditions that are amenable to IVF/ICSI using the man's sperm
- Identify irreversible conditions that are not amenable IVF/ICSI thereby sparing couples the distress of attempting ineffective therapies.
- Identify life-threatening or harmful conditions that may be contributing to the man's infertility
- Identify genetic abnormalities that may affect the health of offspring. Doing so may allow couples to be informed about the potential to transmit genetic abnormalities and may allow a better understanding of the basis of their infertility
Medical History
Questions that are asked during the initial evaluation may pertain to:
- Sexual history (Does the couple have intercourse at the right time of the month? Are they using any vaginal lubricants?)
- Pregnancy history (Has he ever initiated a pregnancy before, either with his current partner or a previous partner?)
- Current therapy (Has he already been treated by another physician or provider?)
- Childhood diseases (Has he had any childhood conditions that may put him at risk for infertility?)
- Medical or surgical problems (Does he currently have any medical conditions or has he had any surgeries that might affect his reproductive potential?)
- Gonadotoxins (Are there any environmental exposures that are putting his sperm at risk?)
Physical Examination
A comprehensive examination by an experienced clinician is critical. Emphasis is placed on the genito-urinary examination including:
- Location of the urethral meatus
- Testis size, consistency, and location
- Presence of varicocele
- Presence of abdominal or inguinal scars
- Presence of vas deferens
- Epididymal congestion
Laboratory Evaluation
In general, 2 separate semen analyses and a routine hormone profile (blood tests) are recommended as part of the initial evaluation.
Basic semen analyses typically report the volume of fluid, the sperm count, and what percentage of the sperm seen under the microscope are moving.
Depending on initial test results, more advanced studies may be recommended, and may include tests of sperm morphology, sperm DNA fragmentation, anti-sperm antibodies, and seminal leukocytes (inflammatory cells in the semen).
Genetic tests, such as karyotype, Y-chromosome microdeletion, and cystic fibrosis may also be indicated when men have no sperm in their semen due to sperm production problems (non-obstructive azoospermia) or due to blockages in the reproductive tract (obstructive azoospermia).
Radiographic Studies
When there are inconclusive findings on the physical examination, a testicular ultrasound may be recommended to further evaluate for the presence or absence of varicoceles or other testicular pathology.In the setting of low seminal volume, absence of the vas deferens, or severely impaired sperm motility a trans-rectal ultrasound may be recommended to evaluate the prostate gland and seminal vesicles for evidence of ejaculatory duct obstruction.
Treatment of Male Infertility
The treatment of male infertility depends upon a number of factors including what abnormalities, if any, were identified during the evaluation, as well as the presence of any female factors such as advanced reproductive age.
Because it can take up to 3 months for new sperm to be produced in the testis and travel through the male reproductive tract, any treatments geared towards improving the amount or quality of sperm in the semen will take time.
Oftentimes, treatment of male-factor infertility requires the expertise of female fertility specialists who perform intra-uterine inseminations (IUI) and IVF/ICSI.
Thus, the optimal treatment of infertile couples requires a coordinated effort between male and female fertility experts to come up with indiviualized treatment plans that fit their emotional, temporal, and financial needs. Support of the emotional needs of both the man and the woman during this time is as important as any medical and/or surgical treatments involved in their treatment.
Common treatments of male infertility are listed below:
Microsurgical Varicocelectomy (see below)
Hormonal Therapy (such as clomiphene or anastrazole)
Anti-inflammatory Medications
Transurethral Resection of the Ejaculatory Duct
Electroejaculation
Microsurgical Varicocelectomy
Varicocele is the most common, surgically-correctable cause of male-factor infertility. While at least 15% of all men have a varicocele, they are found in up to 40-50% of men evaluated for infertility issues.
Varicoceles are enlarged spermatic veins that surround one or both testicles. The exact mechanism by which varicoceles can cause impaired sperm counts and/or quality is unknown, but most experts feel that it is due to increased heat around the testicles.
While varicoceles are not known to cause any other health problems, they can be associated with testicular pain and may contribute to low testosterone levels.
When a couple is faced with infertility and the man is found to have a varicocele, microsurgical repair of the enlarged veins is recommended only when the following criteria are met:
1. the varicocele is palpable
2. there is at least one abnormality present on semen analysis or sperm function testing
3. the female partner has normal fertility, or a correctable infertility condition
Microsurgical repair of a varicocele is performed as a same-day procedure and takes approximately 45 minutes to an hour. Risks are minimal but can include pain, bleeding, infection, hydrocele formation, recurrence of the varicocele, numbness at the incision, and testicular injury or loss (less than 1%). Rest and icepacks are recommended post-operatively, and most men take the prescribed pain medication for about 2-3 days before switching over to acetominophen and/or ibuprofen. Men are encouraged to perform light activity for the first 1-2 weeks after surgery. Semen analyses should then be checked every 3 months for at least 1 year or until the couple achieves pregnancy.
Varicocelectomy improves semen quality about 70-80% of the time. Pregnancy results are variable, with studies reporting pregnancy rates of 40-60% within 1-2 years of treatment, compared to 10-15% of couples where the man did not have his varicocele(s) repaired.
The following are intraoperative photgraphs demonstrating the advantages of the operating microscope in visualizing vital structures and safely and effectively repairing a symptomatic varicocele.
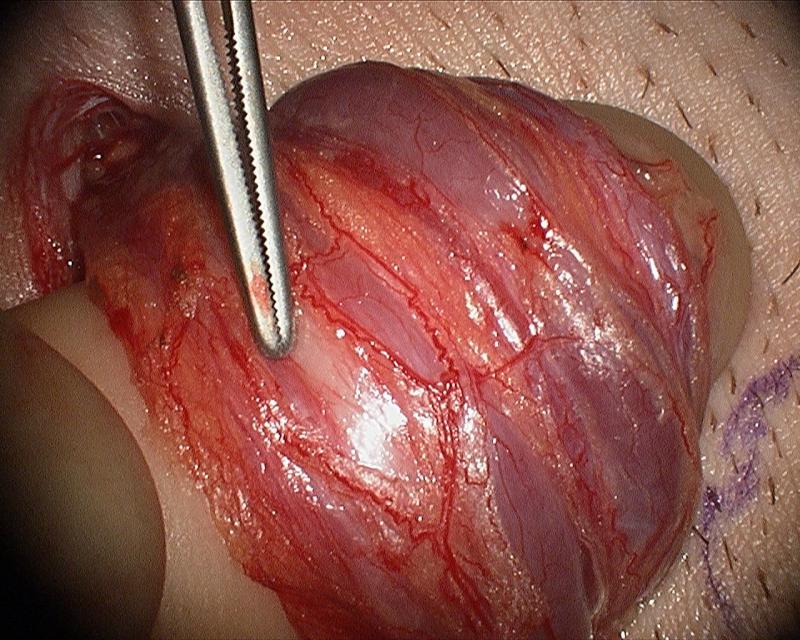
The vas deferens (white) is easily identified and spared.
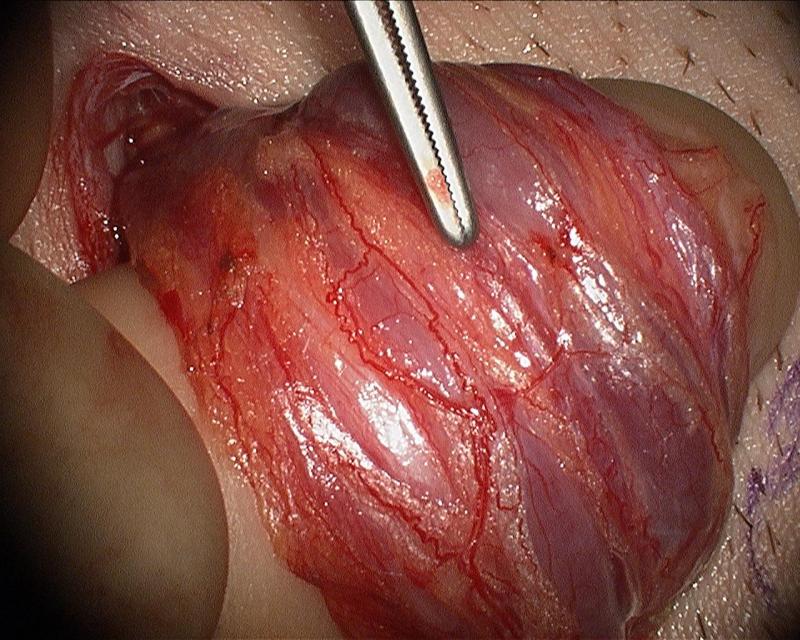
The testicular artery (red, at tip of instrument) is easily identified and spared.
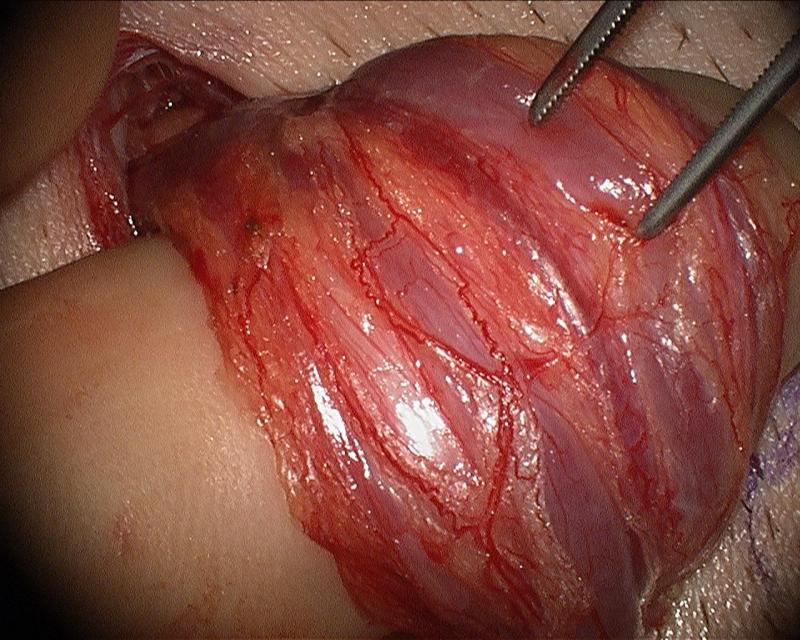
Lymphatic channels (clear structure, next to tip of instrument, next to blue vein) are easily identified and protected.
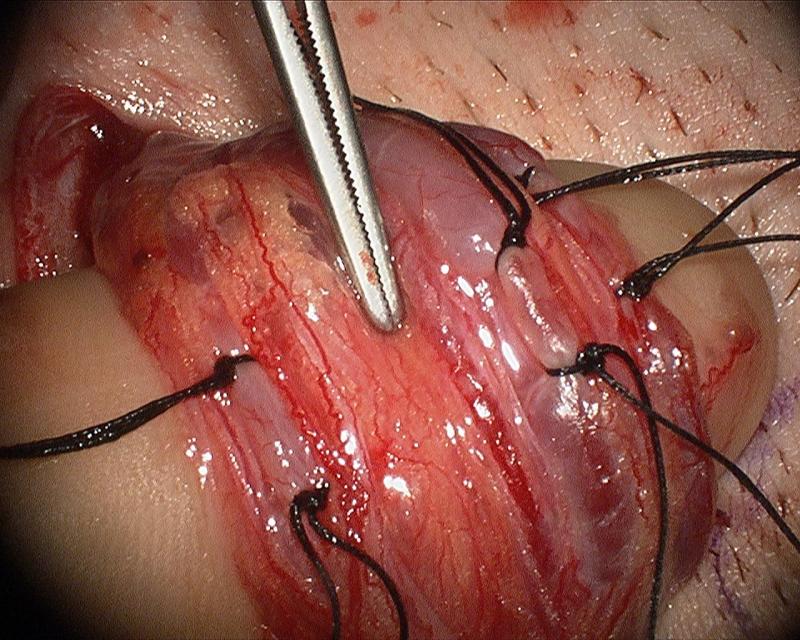 Each vein is doubly-tied with a 3-0 silk suture. Critical stuctures are spared including the vas deferens (to the left of the tip of the instrument), the testicular artery (to the right of the tip of the instrument), and a prominent lymphatic (to the right of the testicular artery, left of the vein that has been tied).
Each vein is doubly-tied with a 3-0 silk suture. Critical stuctures are spared including the vas deferens (to the left of the tip of the instrument), the testicular artery (to the right of the tip of the instrument), and a prominent lymphatic (to the right of the testicular artery, left of the vein that has been tied).
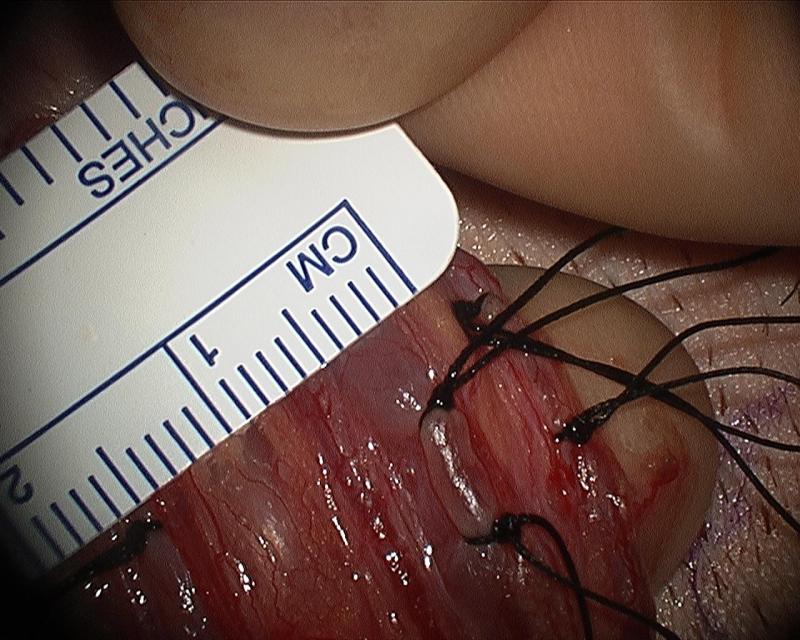 Clinically symptomatic varicoceles measure greater than 3 mm. The vein in this photograph measures 4 mm.
Clinically symptomatic varicoceles measure greater than 3 mm. The vein in this photograph measures 4 mm.Dr. Williams' Article About Microsurgical Varicocelectomy
Click Here to See How Varicocele Repair Improves Male Infertility